











































The Power of Women's and Men's Social Networks to Catalyse Normative and Behavioural Change: Evaluation of an Intervention Addressing Unmet Need for Family Planning in Benin
Patient-Centered Outcomes Research Institute, Clinical Effectiveness and Decision Science (Kim); Georgetown University, Institute for Reproductive Health (Igras, Diakité); University of California, San Diego (Barker, Lundgren)
"Results support the broader use of innovative social and behaviour change strategies that diffuse family planning ideas through social networks, diminish normative and communication barriers, and catalyse modern family planning use."
Programmatic approaches to address the unmet need for family planning (FP) have typically focused on structural factors. Yet, despite the fact that substantial FP programme investments in Benin have resulted in an FP-knowledgeable population and widely available FP services, modern contraceptive prevalence remains relatively low (12%) and unmet need for FP relatively high (32%). In response, the Tékponon Jikuagou (TJ) intervention applied social network theory in an attempt to reduce socio-normative barriers preventing modern contraceptive use in rural Benin. This paper evaluates TJ's effectiveness and examines how intervention components affected intermediate and primary FP outcomes.
Social network interventions work by catalysing social networks - the aggregation of individuals connected by interpersonal relationships - to diffuse new ideas, attitudes, and behaviours. Those playing socially influential roles can be family members (e.g., mothers-in-law and sisters), friends, and community leaders, and these people can influence many areas of health. Social network approaches are anchored in social network and behaviour change theory, which focuses on social relationships in transmitting, influencing, and channeling interpersonal or media influence, as well as enabling attitude or behaviour change.
TJ is described in depth at Related Summaries, below. In short, TJ works with and through existing social groups and opinion leaders to engage women and men in reflection dialogues. These dialogues allow social comparison and learning and promote the diffusion of new ideas to break communication and other social barriers that prevent women and men with unmet needs - those who wish to space their next birth but are not using effective FP methods - from acting on their desires. The steps include:
- Community social network mapping: In each village, 3-5 of the most socially influential women's and men's groups and 5-10 influential opinion leaders of both sexes are invited to become TJ network actors and are oriented.
- Influential group dialogue and critical reflection: Socially influential groups use materials designed to encourage dialogue and critical reflection about gender roles, social norms, and reproductive health issues and then share (diffuse) new ideas with friends and family. These dialogues use communication for social change techniques, which work to empower people and facilitate equitable social transformation.
- Opinion leader engagement and discussions with constituents: Influential opinion leaders use their position in communities to support positive discussions about fertility concerns and FP, breaking down taboos of discussing FP in public.
- Radio broadcasts: Local radio stations reach a larger population with new ideas through re-broadcast of TJ stories and discussions during group meetings.
- Linking of network actors to FP services: Providers meet influential network actors and collaborate with them in a push campaign midway through implementation. The "Each One Invites 3" campaign asks members in influential groups to discuss and then invite non-FP users to seek information and services with an invitation card. Service providers prioritise potential clients who arrive with the FP invitation cards.
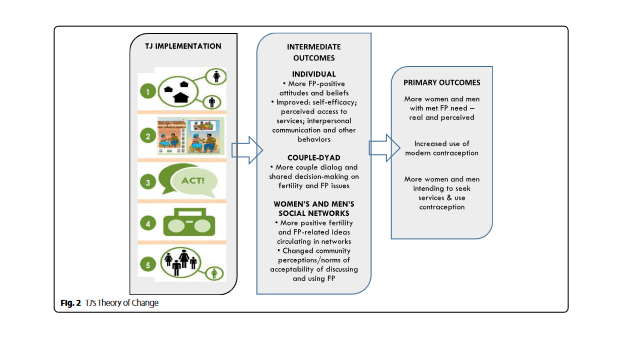
As shown in Figure 2 of the paper, the TJ Theory of Change (ToC - see above) asserts that the five inter-linked programme components will create mutually reinforcing changes by women and men at the individual, couple, and network or socio-normative level. To test the ToC and evaluate TJ's impact on individuals and the broader social network or normative level, the researchers undertook pre/post-intervention cross-sectional research in Benin's Ouémé Department among a comparison group at baseline in May 2015 (1,043 women and 1,030 men) and 14 months later at endline in September 2016 (1,046 women and 1,045 men). Using sex-stratified models, the researchers assessed balance across intervention and comparison groups on background characteristics using Pearson's chi-square tests of independence; they performed bivariate tests of independence to assess differences between baseline to endline on intermediate outcomes and primary FP outcomes; and they used logistic regression to examine the effect of intervention components on intermediate and primary FP outcomes.
The TJ evaluation included four primary outcomes, which were assessed using binary measures of (i) current use of modern contraception; (ii) intention to use a modern FP method; (iii) actual met need for FP; and (iv) perceived met need for FP. Intermediate outcomes included: individuals' self-efficacy and perceptions of ability to access contraception; couple communication on fertility and FP; social network diffusion behaviours including communicating in public about FP and fertility; social network diffusion indicators such as seeking advice from and sharing advice with others; and attitudes and normative beliefs about fertility, FP, and gender.
Statistically significant improvements were found in three of the primary outcomes: women's intentions to use modern contraception, achieve met need, and reduce perceived met need. For example, among women in the intervention areas, modern contraceptive use increased from 31.6% at baseline to 46.5% at endline. This is an 8.6 percentage point increase over the change in the comparison group (19.5% at baseline to 25.8% at endline). Women's intentions to use FP showed a 10 percentage point change (p < 0.05) between the intervention and control groups and actual met need a 21 percentage point increase; p < 0.001) from baseline to endline between the intervention and control groups. Similarly, there was a significant decrease in perceived met need for FP in intervention sites from baseline to endline, compared to comparison sites (-11%; p < 0.001).
Among men, changes were less consistent, though men's achievement of met FP need and reduced perceived met need were statistically significant. The fourth primary outcome, actual use, showed substantial gains, although not statistically significant.
Assessing intermediate outcomes at individual, couple, normative-network levels, TJ led to statistically significant increases in couple and network communication on fertility desires and FP use and self-efficacy and confidence to access services. More specifically:
- Women's results show statistically significant improvements in all but one intermediate outcome - the attitudes and normative beliefs about gender and FP indicator. Statistically significant increases were measured in women's self-efficacy in using a modern method correctly all the time (19%; p < 0.001) and knowing where to obtain contraception (18%; p < 0.001). Similar increases were seen for all couple communication indicators: a 22% increase (p < 0.001) in women who reported they were comfortable talking with their husband about FP use; a 47% increase (p < 0.001) in women saying they discussed with their husband having children in the previous 12 months; and a 43% increase (p < 0.001) in women reporting they talked with their husband about how to obtain a modern FP method in the previous 12 months. Significant increases in social network diffusion indicators for intervention sites were also observed: a 42% increase among the intervention group (p < 0.001) women who said they asked friends or family members about their experiences with FP in the last three months; a 29% (p < 0.001) increase in sharing FP knowledge or positive experiences with family or friends in the previous three months; and a 19% increase (p < 0.001) in women who corrected someone saying something untrue about FP in the last three months.
- Attitudes and normative beliefs about fertility, FP, and gender showed greater variation in results.There was a 20% increase in women reporting it is acceptable to discuss FP in public in their village. The other two indicators of attitudes and normative beliefs moved in undesirable directions.
- Among men, fewer consistent changes were seen in individual and couple-focused indicators, but significant differences were measured in diffusion and normative expectations. For example, there were highly significant increases from baseline to endline in intervention areas compared to comparison sites in men's self-efficacy in using a modern method correctly all the time (10%; p < 0.01) and for knowing where to obtain contraception (33%; p < 0.001).
As shown in Table 4 of the paper, for women, the odds of modern contraceptive use and achieving actual met need were four to six times greater than those not exposed to all types of TJ intervention activities. Overall, the effect sizes were smaller and less often statistically significant for men exposed to the TJ activities than women.
Adjusted odds ratios reveal differing effects. Women involved in interpersonal/group engagement and listening to leader talks were statistically four to five times more likely to use modern contraception, with similar odds ratios seen in women's achievement of met need. Men were most influenced by radio broadcasts, being one to two times more likely to use modern contraception and achieve their met need.
Notably, TJ aimed to shift community norms about FP. The adjusted odds ratios for attitudes and normative beliefs about fertility, FP, and gender confirmed this shifting. TJ influenced what individuals perceived about what others were thinking and doing (descriptive norms) and should be doing or not doing (injunctive norms) in their networks.
In sum, by endline, after 14 months of implementation, statistically significant improvements were seen in women's intentions to use modern contraception, achieve their met need for FP, and reduce perceived met need (less were erroneously believing to be protected from unplanned pregnancy). Women showed substantial gains in actual use, but the difference was not statistically significant. Men's achievement of met need for FP and reduced perceived met need were also statistically significant. The intermediate outcomes that encourage such movements by women and men all improved.
In conclusion: "The TJ approach shows that participation of a small set of influential network actors, coupled with public discussion and diffusion of new ideas raised through reflective dialogue, can reach large populations, representing a low-resource and low-technology FP promotion package. Ultimately, an approach like Tékponon Jikuagou's may be an effective way to improve FP uptake by tackling a core but a poorly-addressed problem in many FP programs: the socio-normative barriers to women and men acting on their unmet need."
BMC Public Health (2022) 22:672. https://doi.org/10.1186/s12889-022-12681-4
- Log in to post comments