











































Critical Success Factors for Routine Immunization Performance: A Case Study of Zambia 2000 to 2018
Emory University (Micek, Hester); Center for Family Health Research in Zambia (Chanda) - plus see below for full authors' affiliations
"...findings support the conclusions of others in ensuring optimized vaccination efforts including, political backing and investment, prioritizing vaccine equity, community-tailored approaches, and increased demand..."
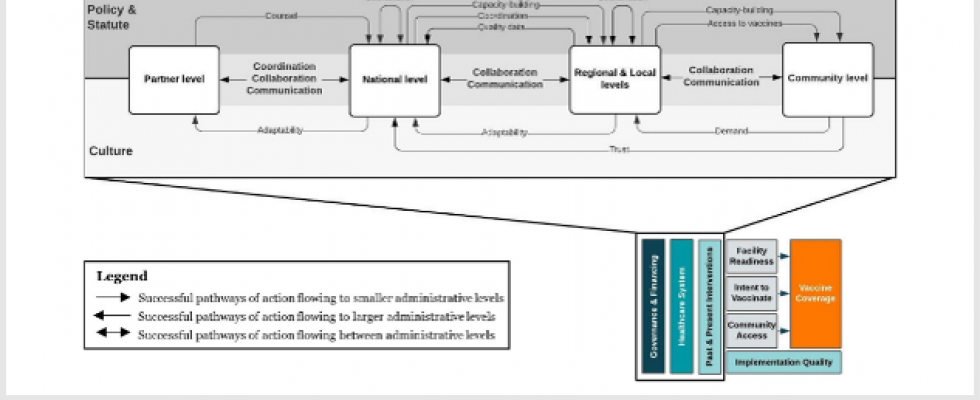
Zambia has maintained consistently high coverage of the first dose of diphtheria, tetanus, pertussis vaccine (DTP1) since the early 2000s. This study uses a positive deviance case study methodology to identify and understand policies, programmes, and other contributing factors that influenced high coverage rates in Zambia from 2000-2018. The researchers modified an existing evidence-based conceptual framework that describes the core requirements for vaccine systems, exploring additional facilitators and barriers to vaccine coverage at national and subnational levels. The framework incorporates demand- and supply-side components to ascertain success factors and their implementation strategies. The study's results shed light on the multidimensional components that are critical to an effective immunisation programme.
Qualitative data were collected between October 2019 and February 2020 at the national, provincial, district, health facility, and community levels in: Chongwe, Lusaka, and Rufunsa districts in Lusaka Province; Chibombo, Chitambo, and Serenje districts in Central Province; and Chipili, Nchelenge, and Samfya districts in Luapula Province. Key informant interview (KII) and focus group discussion (FGD) guides were informed by the Consolidated Framework for Implementation Research and the Context and Implementation of Complex Interventions framework. KIIs were conducted at national (N = 22) and subnational (N = 45) levels; 21 FGDs were conducted with community-based volunteers, or CBVs (N = 10), mothers (N = 8), fathers (N = 1), and grandparents (N = 3).
Through KIIs and policy reviews, the researchers identified several government policies, health campaigns, disease outbreaks, natural disasters, and key interventions that may have affected immunisation coverage in Zambia from 2000 to 2018. The following success factors emerged:
- Initially created in the 1990s by the World Health Organization (WHO) as a country-level working group to coordinate polio eradication, the Inter-agency Coordinating Committee was strengthened for long-term engagement, which, complemented by the Zambia Immunization Technical Advisory Group, is valued by the government and integrated into national-level decision-making. Alignment of priorities towards a common strategic vision enhanced vaccine programme performance.
- The Ministry of Health (MoH) improved the coordination of data collection and review for informed decision-making across all levels. Frontline health workers gained localised ownership of decision-making through the routine collection and review of community data. To improve and sustain the quality of data reporting and management, the Monitoring and Evaluation Department at the national level provides trainings to staff at all levels on health information systems and tools. Integrated meetings for data review are held at the district and provincial levels monthly and quarterly, respectively.
- Regional multi-actor committees identified development priorities, strategies, and funding and iteratively adjusted policies to account for facilitators, barriers, and lessons learned. Through decentralisation, while the MoH at the national level focuses on policymaking, implementation and management of immunisation programming shifted to the subnational levels. The Zambian model to promote collaboration and communication between levels includes the District Development and Provincial Development Coordinating Committees. Ultimately, providing an opportunity for iterative adaptation of policies improved subnational and community stakeholder ownership of programme planning, implementation, and concordance across levels.
- The Zambia Vision 2030 policy laid the groundwork for a partnership with the media (e.g., television, radio stations) and described information as a "resource" critical for socioeconomic development. Vaccine messaging was disseminated through multiple channels, including the media and community leaders, increasing trust in the government by community members. Provincial and district health officers, and occasionally community leaders, were invited to local radio stations and were provided free airtime several times per year to discuss immunisations. This arrangement provided the media with the influence to dispel myths and misconceptions related to vaccinations. Open communication between community leaders and MoH officials at the district and regional levels shaped community views on vaccines. The key development and health policies in Zambia reference training and engagement of community leaders as essential components of vaccine delivery. Both community leaders and subnational ministry officials noted that vaccine delivery has always required the approval and participation of traditional leaders, who act as gatekeepers to their communities.
- The MoH and Churches Health Association of Zambia (CHAZ) formalised a long-term organisational relationship to leverage the strengths of faith-based organisations. CHAZ is involved at the national level in immunisation message development for the general population and the media, especially during the introduction of new vaccines and Child Health Week. CHAZ develops and presents concept notes for message development and delivery to the immunisation technical working group to review and revise. CHAZ also has a champion programme in which it identifies and trains media and community members to disseminate immunisation messaging to reach minority religious groups. Finally, CHAZ works with community organisations and health facilities to ensure equitable health outreach and service provision across Zambia
- Neighborhood Health Committees (NHCs), a group of CBVs in communities in Zambia, spearheaded community-driven strategies via community action planning and ultimately strengthened the link between communities and health facilities. For example, NHCs worked with health facility staff to develop the outreach timetable, communication plan, and local leadership engagement plan. Tailored outreach messaging was used to address hesitancy in community members, and NHCs and other frontline outreach workers provided health education to inform community members on the benefits of vaccines. In Zambia, community members respect NHCs due to their appointment by community leaders and their link to the health facility in planning, evaluation, communication, and coordination.
Based on the findings, the paper outlines some implications for investments in immunisation programming. For example, Zambia's policies and statutes include some flexibility in implementation to allow for tailored outreach approaches in each district to identify and expand services to hard-to-reach populations, which influenced the communication and collaboration between levels. Areas with lower coverage should - and did - have increased allocation of resourses and interventions.
Regarding the study's methodology, the researchers comment that, "Applying a positive deviance lens to the relative contributions of these essential health system components to increases in immunization coverage may identify transferable lessons and support actionable recommendations to improve national immunization coverage and increase vaccine equity..."
In conclusion: "The experience in Zambia suggests that targeted vaccine interventions may have a short-term impact, but the sustainability of the immunization program is supported by consistent and reliable coordination, collaboration, and communication between the government, community, and partner networks as strengthened through health system reform. Deriving the key elements of these networks and how each contributed to immunization program performance is critical to determining how and why vaccine coverage improved in a specific context."
Full list of authors, with institutional affiliations: Katie Micek, Emory University; Kyra A. Hester, Emory University; Chama Chanda, Center for Family Health Research in Zambia; Roopa Darwar, Emory University; Bonheur Dounebaine, Emory University; Anna S. Ellis, Emory University; Pinar Keskinocak, Georgia Institute of Technology; Abimbola Leslie, Emory University; Mwangala Manyando, Center for Family Health Research in Zambia; Maurice Sililo Manyando, Center for Family Health Research in Zambia; Dima Nazzal, Georgia Institute of Technology; Emily Awino Ogutu, Emory University; Zoe Sakas, Emory University; Francisco Castillo-Zunino, Georgia Institute of Technology; William Kilembe, Center for Family Health Research in Zambia; Robert A.Bednarczyk, Emory University; Matthew C. Freeman, Emory University; and the Vaccine Exemplars Research Consortium
Vaccine: X, Volume 11, August 2022, 100166.
- Log in to post comments